

Saturday, October 21, 2006
Elderly patients' understanding of CPR outcomes; Pallimed layout changes?
I)
The July issue of the Journal of the American Osteopathic Association has a research article on elderly patients' understanding of CPR survival (available in free full-text at least as of today). 100 elderly (over 70 years old) patients at a single institution were asked (in non-medical language) what they thought their chances of survival-to-discharge would be if they needed CPR while hospitalized. The patients were also asked if they had a pre-existing DNR order and where they get most of their medical information from. The results were:
1) Over 80% of respondents thought they had better than a 50% chance of survival to discharge (see figure).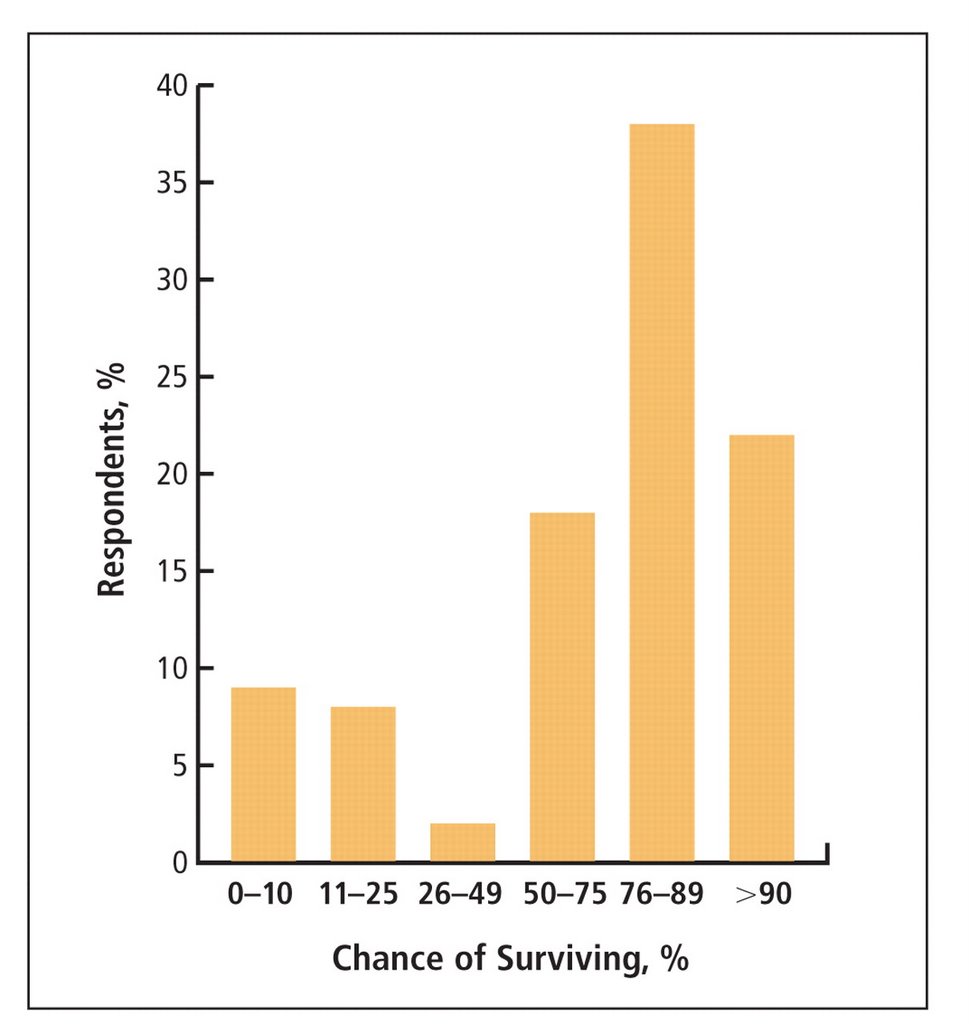
2) More patients reported they got most of their medical information from television than from their physician.
A couple of things here. This was the first research article I've ever read in JAOA and was disturbed to find it lacking in many of the elements which we expect in a research article to give it at least a verneer of authenticity and scientific validity. A few examples:
a) We are told that 70 elderly people at this institution were "chosen randomly" from the inpatient wards, the ER, and primary care clinics; we are never told how these people are actually chosen & for all we know a researcher walked around with a pad & pencil and 'randomly' selected old looking people for the study.
b) The article doesn't include the nearly-ubiquitous "Table 1" describing basic demographic and clinical details of the subjects. We really have no clue who these people are other than their age category and they were sitting around this medical center one day.
c) The most basic of statistical analyses are absent, including the most obvious analysis looking to see if having a pre-existing DNR order or living will was correlated with a more accurate assessment of CPR survivability or not. I'm not asking for a complicated multivariate analysis here--they had the data to answer this simple question but didn't I guess bother to do it.
All of this is quite frustrating, limits the impact of this sort of research, and all together seems like a squandered opportunity.
Pious criticism aside, their findings are certainly grossly accurate (people greatly overestimate the benefit of CPR) and you've got to wonder if it would be a worthwhile public service campaign to educate people just how ineffective this procedure is in most sick, hospitalized patients. Unlikely to happen, & as I think about it unlikely to make a difference either. There will continue to be those (thankfully rare) patients and families for whom anything other than maximum medical intervention will be seen as giving up or somehow giving in to death. Most patients/families aren't like this, and with a straightforward discussion of ways to be cared for as they die, along with a physician recommendation to not undergo resuscitative efforts, they will be agreeable to a DNR order. In medicine we can't change what's on TV, but we can change how, and how often, we talk with patients about these matters. The problem, of course, is that as a profession we do this very poorly, and "code status" discussions--when they occur at ll--are often no more or less than an intern asking a patient "If your heart stops do you want us to restart it?" Put that way, I'd say "Yes" too.
II)
In the near future I am going to try to upgrade Pallimed to the a new version of Blogger that Google/Blogspot are developing. Hopefully this will be smooth and improve the whole Pallimed experience. It may also be a consummate disaster and force me to do a revert back to the old Pallimed, etc. etc. The point here is that if things are wacky, absent, or broken for a few days that's why. I'm asking your forgiveness in advance....
--Drew.

