

Tuesday, January 31, 2006
The current Journal of Clinical Oncology has a couple articles to note.
First, there is a discussion of recommendations for breaking bad news. It is based on data that is being gathered for a larger trial about communication in oncology clinics, and uses information coded from video-taped encounters between oncologists and patients. The authors present their discussion against a straw-man of pre-existing 'guidelines' about breaking bad news which they suggest are overly simplistic. Obviously they are overly simplistic--that's the nature of guidelines--but the authors' observations about how bad news unfolds in the clinical encounter are nonetheless interesting and useful. First, they observe that 'bad news'--defined as " [news that] results in a cognitive, behavioral, or emotional deficit in the person receiving the news that persists for some time after the news is received"--comes out all the time in routine clinical encounters (not just in the You Have Cancer or You Are Dying talks). Second, they point out that to patients and families there's sometimes not a central Bit of Bad News, but rather several (3.2 on average per encounter, actually!) pieces of 'bad' information that come out in an encounter. Finally, they observed that a physician-patient dyad doesn't really exist, and that family members often contribute as much to the encounter as patients or docs. None of this is earth-shattering; but it's interesting to see data taken from actual physician-patient-family interactions. I'm not clear what the goal of the larger trial is, but based on this preliminary missive, it seems that its results may be quite interesting. I guess we'll wait and see.
Additionally, a randomized-controlled trial about a multidisciplinary intervention to improve the quality of life for 'advanced' cancer patients is presented. This was a trial at Mayo for patients with advanced cancer (defined as life expectancy longer than 6 months but mortality at 5 years thought to be over 50%) undergoing radiation therapy. The treatment group received a multidisciplinary intervention (8 sessions, 90 minutes each, over 3 weeks) comprising physical therapy, chaplaincy services, and broad ranging cognitive-behavioral-emotional education and support. Essentially, the intervention group did a little better quality-of-life-wise at 4 weeks but this quickly petered out; mostly this benefit was in stopping the decline in quality of life during radiation treatment that the control group experienced. See the figure below...despite statistical significance not a very impressive response.
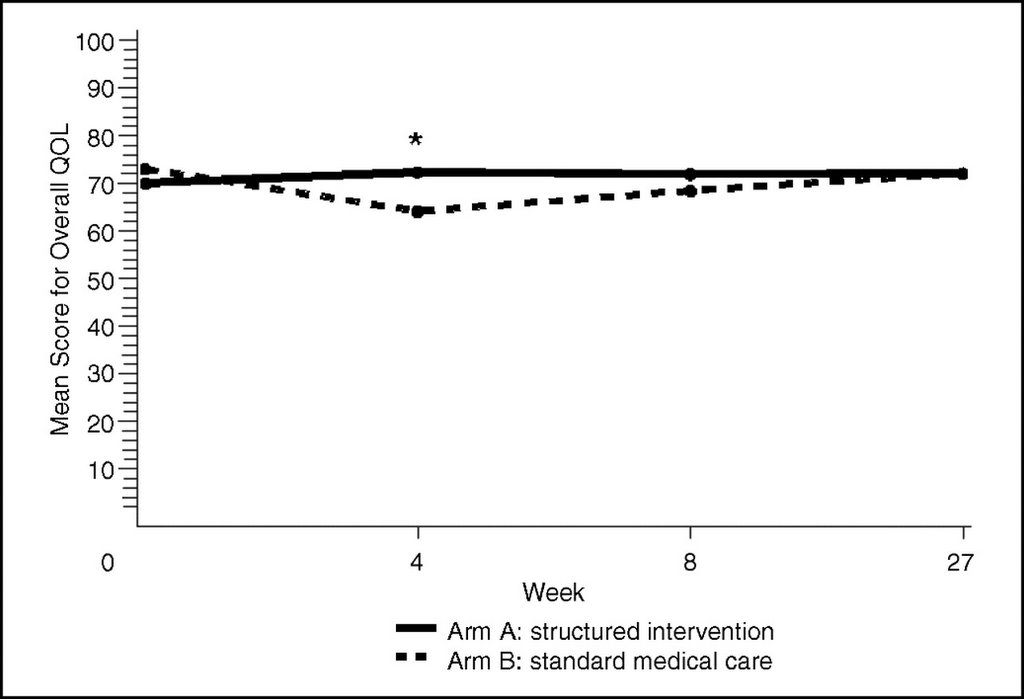
This is one of those articles that if you read the abstract you get the feeling that this was a solid success, whereupon reading the text you realize that it the intervention's benefit was modest (at best) and transient (and at what cost?). My gloss on this is that the problem may be one of selection--services like this are probably only helpful for a subset of patients and the trick may be in figuring out which ones. Part of what I'm suggesting is that for many patients 'quality of life' is adversely affected by so many things that these sorts of interventions just can't address. Having advanced cancer sucks (as many buttons worn by staff at the cancer center I work at attest to); it makes you feel crappy and usually eventually takes everything meaningful away from you including your life. Benefits aside--cancer treatment, radiation included, also sucks and makes you feel crappy while you're undergoing it. Will having sessions discussing body image and stair exercises make this suck any less? For many people clearly not; the trick is to identify those for whom it would help.
(& I did listen to the Fresh Air bit from earlier this week & it's quite good: a short, fluent, and sometimes personal account of geriatric and end of life care in 21st century America.)
Tuesday, January 31, 2006
A quick basic science fix:
The Journal of Internal Medicine has a review on opioids in critical illness. Specifically, it is about the complicated hemodynamic, endocrine, and immunologic effects of endogenous and pharmacologic opioids on the response to critical illness (hemorrhage, sepsis, surgery, etc.). Ultra brief summary: rat studies suggest opioids attenuate the counter-regulatory response to critical illness in bad ways, so are we doing harm by using them in the ICU? There's no answer to this of course, but a plug for ketamine as a hypothetical counterbalance to this hypothetical danger is mentioned.
Also...
Gastrointestinal Endoscopy has published a review on feeding tubes in people with advanced illnesses. James Hallenbeck wrote an accompanying editorial & discusses it in his blog at Growth House.
According to my wife, during today's Fresh Air radio show on NPR about Medicare Part D with Dr. Christine Cassel from the American Board of Internal Medicine, they venture into discussing end of life care in the hospital (& the great need for improving it in the US). You can listen to the show on-line if you miss the broadcast.
Sunday, January 29, 2006
Some excerpts from 2 (two!) Fed Ex letters I received from Valeant Pharmaceuticals:
As a recognized leader in Palliative Care you have been specially selected to particpate in a Consultant Forum. The focus...is to understand the current perceptions towards Cannabinoids and their potential...
Now I thought that was nice that they complemented me. Made me feel good. A recognized leader. Not bad for being two years out of fellowship. Hmmm..the current perceptions towards Cannabinoids. More on that in a bit.
Consultant Forum particiapants will be provided a consulting honrarium of $500 from Valeant Pahrmaceuticals. ...will be held at Ruth's Chris Steak House in Nashville...in conjunction with the AAHPM 2006 Annual Assembly.
Wow! That is a lot of money. In fact very close to the amount for the whole assembly. 3 days of educational talks and I have to pay over $500, but then I could also receive $500 for helping advocate for cannabinoids in the United States.
Well since you already know my opinion on pharmaceutical industry and honorariums, (I don't like them and vow not to take any pens or 'free lunches.') you already know I was not going. I will be going to the Grand Ol' Opry that night on my own dime though!
So I did a little digging. Valeant Pharmaceuticals is based out of Costa Mesa, CA and is the maker of Cesamet (nabilone) an anti-emetic based on the cannabinoid class. My first letter was received in early January. Five days after the FDA denied Valeant changes in labeling.
What those changes were are not clear, but Valeant is not putting Cesamet on the market until further discussions with the FDA. Well Cesamet is on the market in Canada where it controls 88% market share. The drug was originally developed by Eli Lilly, but never went to market in the US when it was apparoved for Chemo induced nausea and vomiting in 1985.
So where am I going with all this?
Nabilone itself looks like it may be an effective antiemetic per this report in BMJ in 2001 (pdf) (no declared competing interests). I have no problem advocating for more effective medications for palliative care. My problem is the way this is done. I may end up advocating for this medicine, but I do not feel like I need to get paid $500 or get a nice steak dinner for it. Why not more discussion among oncologists if they feel they have no effective tools for chemo induced N/V? Why not more presentations at conferences that are open to scrutiny by peers and without funding from the pharma?
I want everyone to understand I have nothing personal against nabilone, cannabinoids or Valeant Pharmaceuticals or the FDA. I believe this is all part of the dance of the current system and it is unfortunate it has to be this way.
I know my question at the Assembly will be: Hey you going to Ruth's Chris on Friday night?
PS: Like the name: Cesamet (Cease + Emesis OR Cease + Mets)
Sunday, January 29, 2006
 For the Pallimed readers who are not board certified with the ABHPM, just a reminder that 2006 is the last year until 2008 to get certified before the American Board of Medical Specialties begins oversight.
For the Pallimed readers who are not board certified with the ABHPM, just a reminder that 2006 is the last year until 2008 to get certified before the American Board of Medical Specialties begins oversight.
The test dates are Nov 4-11 (one day only)
The fee is $1100 if you register by April 1, 2006. Last day to register is May 31, 2006.
See the ABHPM website for more details depending on your specific situation.
Saturday, January 28, 2006
Another e-publication ahead of print from Supportive Care in Cancer...
Our colleagues at the Cleveland Clinic have compared the systematic assessment of patient symptoms to relying on patient reporting of symptoms. They looked at 200 patients referred to their service (the vast majority had cancer; 44% were inpatients). The patients were initially asked two open ended questions about symptoms to see what they volunteered, and then underwent a directed, systematic assessment of 48 symptoms. This is a well done, important, and provocative study.
First off, this gives us a valuable look at symptom burden in a cohort of patients referred to a palliative care service, albeit at a single institution. The top 12 symptoms found, in descending order, were fatigue (73%), dry mouth (67%), pain (64%), anorexia (59%), weight loss (54%), early satiety (49%), insomnia (43%), dyspnea (43%), drowsiness (41%), constipation (39%), cough (39%), and depression (36%). Not surprisingly, the more severe or distressing the patient rated a symptom, the more likely s/he was to report it. However, and this is probably the most important finding of the study, several symptoms were rarely volunteered even if the patient rated them "distressing" when specifically asked about them. This included fatigue (42% volunteered this symptom), anorexia (31%), and early satiety, dry mouth, insomnia, and weight loss (all less than 10%). Likewise, several symptoms which the patients rated as "moderate" or "severe" (even if not "distressing") were rarely volunteered--these included fatigue, dyspnea, early satiety, drowsiness, dry mouth, insomnia, and weight loss.
Does this mean all patients should have directed, systematic, and exhaustive symptom assessments? I don't think so, but you could use these findings to argue with me. Probably very few of us when interviewing patients rely solely upon patient volunteered symptoms, and a good 'review of systems' is integral to every--at least initial--patient assessment. So whether systematic assessment actually offers the patient anything more than routine care is unknown. This assumes of course that routine care is good care, but that's another story. What would need to be demonstrated is that systematic assessment offers patients some benefit--quality of life, symptom improvement, satisfaction with care, etc. There's also the question of burden to the patient of exhaustive interviewing, not to mention the time-cost and practicality of this outside of the research setting. Also, what is one to make of symptoms that patients, when asked, say are distressing or severe, but that previously they didn't bother to offer. Some of these are probably symptoms that patients have resigned themselves to as inevitable, even if they aren't, and these are the ones that we could make an impact on with systematic assessment (or a thorough history taking!). One wonders though, despite being reported as 'distressing,' how many of these symptoms were making a substantial negative impact on the patients' quality of life in this study? Are these research-generated symptom incidentalomas? Nevertheless, clearly it's a good idea to be on the look-out for those under-reported symptoms mentioned above.
Saturday, January 28, 2006
Thursday, January 26, 2006
Supportive Care in Cancer has e-published a short article about using gabapentin for sweating in cancer patients. It presents a case-series of 9 patients with advanced cancer and severe sweating (which they rated on a 0-10 numeric rating scale); all of the patients had "idiopathic" sweating ( i.e. none had neuroendocrine tumors or were receiving hormonal therapies etc.). All patients had a good response to a week of gabapentin (at least a halving of their sweating rating) with tolerable side effects. Doses ranged from 600-1800mg a day. All these patients were inpatients on a cancer ward presumably receiving other treatments and so, along with simple regression-to-the-mean, more study is needed to say to least. But this is promising, and adds to the slowly mounting evidence that gabapentin has efficacy for a variety of symptoms besides neuropathic pain.
Thursday, January 26, 2006
Wednesday, January 25, 2006
JAMA published an article on health professionals interactions with the pharmaceutical and medical device industries today and it is already making some of the news talk show circles. After discussing recent congressional hearings, and lawsuits against the pharmaceutical industry crossing ethical boundaries, the article focuses on the role of academic medical centers (AMC) and the need for larger reform from the physician side of the interaction. They state that AMCs are influential to the surrounding community and that training physicians learn their practice patterns there and should be free of biased influence.
Now, for anyone who has been in training you are very familiar with the cries of..."It's just lunch" "I won't prescribe that JUST because they gave me a pen." And my favorite of all, "I'm too busy (read: lazy) to get my own lunch, pen, etc." So the article goes on to state what construes a 'conflict of interest.' Here is their list of issues to be addressed:
The authors note there are guidelines but they are not in complete agreement nor are they stringent or enforced. So they call for more rigorous guidelines such as 1) NO GIFTS, MEALS, TRAVEL, OR CME regardless of amount; 2) vouchers for low-income patients instead of samples; 3) exclusion of health care professionals from formulary committees if they have any financial relationship with industry; 4) elimination of Speaker's Bureaus; and 5) funneling travel through a central office at the AMC.
- Gifts (even small value)
- Meals
- Payment for attending conferences and lectures - 314,000 sponsored events for physicians in 2000
- Payment for online activities
- Free CME
- Payment for travel to meetings
- 'Scholarships' for meetings
- Payment for Speakers Bureau participation - Hundreds (if not thousands) of physicians on advisory boards or speakers bureaus
- Providing ghostwriting services
- Providing free drug samples
- Payment for 'consulting services'
- Grants for research projects
They also have a great section explaining the 'myth of the small gift' and the principle of reciprocity regardless of the size of the gift. They even quote research stating the motive of gift-giving is to receive back in return regardless of situation (birthdays, anniversaries, etc.)
Now as you may be able to tell, I am not a large fan of this aspect of medical and pharmaceutical interactions. I have seen misconduct in regards to these interactions, and whenever I try to set an example I have been ridiculed, such as when I brought/purchased my own lunch during residency, while other residents dined away on 'drug rep food.'
In the effort of full disclosure I have received money from a drug company in 2004 to give a talk on pain control in Las Vegas. I did it once, and determined I would not do that again. There was no undue pressure, but I just came home feeling obligated to the drug company. And I hate the excuse I hear from some docs of "Everybody else does it so I'll just do it a little bit."
Luckily, the palliative medicine field is not inundated with drug reps and device companies, but I have a feeling that may change in the future. Last year at the AAHPM talk a lunch symposium was held touting the benefits of Palladone (long acting hydromorphone), which has since been withdrawn from the market (07/05). Many people I spoke with at the Assembly were dismayed at such a blatant 'detailing.' Should organizations like AAHPM and NHPCO join JAMA in proclaiming no more gifts? No Free Lunch?
I think so. I am too proud to take someone's free pen, when I can buy my own.
Wednesday, January 25, 2006
Tuesday, January 24, 2006
The American Journal of Medicine this month has a review on the management of psychiatric problems in critically ill patients. It is a well written, practical, no-nonsense review that would be good teaching material for residents and other trainees. That is swell, but not why I decided to blog it. Despite its title and ostensible subject matter, it actually devotes a substantial amount of its text to staff stress stressburn-out in the ICU--this got more column space than depression! What is the world coming to when someone writing a review for the AJM on patient problems in the ICU decides that staff stress and suffering are worthy of mention? Maybe medicine in the 21st Century will be a bit saner the the last....
Tuesday, January 24, 2006
Monday, January 23, 2006
The current Archives of Internal Medicine has an evaluation of the California CHIPS program. This is a California "version" of the nationwide CAPC program to help establish hospital-based palliative care services. The article is essentially a survey of CHIPS graduates; the results support the idea that CHIPS has been helpful in establishing palliative programs at California hospitals. Hospitals were more likely to succeed in establishing a palliative service if they had a preexisting hospitalist service. This isn't terribly surprising, and one wonders if the future of hospital-based palliative care consultation, at least for non-academic institutions, depends on the good work of our hospitalist colleagues.
What's somewhat surprising about this article is that it was published in one of the more prominent general internal medicine journals & not, for instance, the Journal of Palliative Medicine . The actual 'findings' of the survey are probably of very little interest to the average Archives reader. One has to conclude-- the accompanying hurray for palliative care editorial bolsters this conclusion--that the editors of Archives made a decision to promote palliative care by highlighting a program to help expand palliative care services. And that is good news.
The entire issue is somewhat interesting, especially from a research methods standpoint. There's quite a provocative article asking why, given the dozen or so randomized controlled trials (and half as many meta-analyses) on using N-acetylcysteine to prevent contrast nephropathy, do we still not know if NAC actually does prevent contrast nephropathy! One of the answers, interestingly enough, is that this may be such an easily studiable phenomenon (NAC is cheap and safe and practically everyone who walks into a hospital gets iodinated contrast) that it invited a flurry of small, heterogeneous, and under-powered studies.
Finally, there's an analysis of "placebo-induced" side effects in clinical trials which questions how reliable these are to determine baseline adverse events in drug trials.
Monday, January 23, 2006
Sunday, January 22, 2006
I wanted to highlight an article from this month's Supportive Care in Cancer which looks at opioid switching for those not responding to morphine. The study prospectively followed ~200 people started on morphine for cancer pain. If patients were having 'intolerable' side effects or weren't responding to morphine despite usual titration they were switched to oxycodone. Criteria to switch were not clearly or objectively defined--essentially relying on clinicians' judgments about what were intolerable side effects or 'unresponsiveness.' (This is good in that it captures a real life situation well, but limits the ability to repeat this study or interpret what was done if one doesn't know how the decision to switch was actually made.) About 1/4 of the patients underwent a switch.
The good news is that the vast majority--90%--of patients who were switched had a good analgesia/side effect outcome after switching to oxycodone (a few ended up on methadone or fentanyl). This is validation of the long standing and widely accepted practice of opioid switching. I appreciate research like this: looking, in a prospective and relatively controlled way, at the natural history of something everyone does to see if it actually helps & makes sense. It's welcome news that it does help, and it would have been unsettling and actionable news if it didn't.
The bad news is that I'm not sure if we learned anything else from this study, and it raised more questions than it answered. Not surprisingly people who were switched had higher average pain levels, worse worst pain levels, and more severe side effects than those who weren't switched. However, people who switched had lower average morphine doses and lower serum levels of morphine -3- and -6- glucuronide than those who didn't switch. It doesn't make much of a difference, but one wonders if some of the people who were switched were just being underdosed on morphine. Conversely, one could ask if there were genetic/pharmacologic reasons (cytochrome P450 polymorphisms, drug interactions) that lead the switchers to have lower M3G and M6G levels leading to worse analgesia. The authors didn't divide out those who switched for pain control vs. intolerable side effects so it's impossible to know. Oh well. The authors also looked at patient characteristics to see if anything predicted who would be a switcher. The results are curious, to say the least. They found the following baseline characteristics predictive of who would switch: higher weight; use of beta-blockers, proton pump inhibitors, and antiseritonergic antiemetics; higher wbc count; recent chemotherapy; and having a lower GI malignancy. My gloss on this is that those with a higher symptom burden at baseline were more likely to 'fail' morphine due to side effects, but who knows.
(The issue also publishes the results of a non-placebo controlled preliminary trial indicating that prophylactic fluconazole may dramatically reduce the rate of radiation mucositis.)
Sunday, January 22, 2006
Saturday, January 21, 2006
The Lancet has an interesting piece on developments and controversies in the treatment of depression. It initially covers more heavy-duty basic science literature (fMRI, gene studies, etc.), but then enters more familiar territory reviewing psychological therapies, drugs, and non-drug treatments such as electroconvulsive therapies. The concern for increased suicidality with SSRI's is addressed: overall the authors conclude that while it is clear that suicidal thoughts increase early on in SSRI treatment, there's no strong evidence that actual suicides do.
The most interesting part of the piece for me was a brief discussion of SSRI withdrawal symptoms (which are apparently most common with paroxetine and venlafaxine, presumably due to their shorter half lives). Like I blogged previously, there seems to be some unease within the psychiatric community about using the term "withdrawal symptoms," substituting instead "discontinuation symptoms" or "syndrome," to avoid associations with drug "addiction."
And for a hint of what may yet come, brain stimulation therapies (yes with electrodes among other things) are discussed. I am looking forward to these hunks of hardware showing up on my patients. If they haven't already, someone should write an article on up and coming device therapies and implications for end of life care as they are becoming more and more widespread (not only defibrillators but ventricular assist devices, diaphragmmatic "pacemakers," etc.). These are life-saving, but they are going to make end of life decision making even more complicated than it is now. This is fine of course, that's why we do palliative care, but I get a little nervous when I hear about LVADs being used as a "definitive" (or should I say "terminal") therapy for advanced CHF, as opposed to being a "bridge" to transplant....
Some shameless self-promotion: Two Fast Facts that I wrote have now been published on EPERC's website--numbers 147 and 148--on oropharyngeal candidiasis and the lidocaine patch. They are both well-written, insightful, and beyond reproach (ha ha).
Saturday, January 21, 2006
Friday, January 20, 2006
Annals of Internal Medicine has published a "Perspective" on pain management for those receiving methadone or buprenorphine maintenance therapy for opioid addiction. The bulk of the article is dedicated to dispelling the myths surrounding pain treatment for those with substance abuse problems, including:
1. The maintenance opioid agonist provided analgesia,
2. Use of opioids for analgesia may result in addiction relapse,
3. The additive effcts of opioid analgesics and maintenance therapy may cause respiratory and CNS depression, and
4. Reporting pain may be a manipulation to obtain opioid medications, or drug-seeking, because of opioid addiction.
Additionally, it has very focused and practical advice on the treatment of acute pain for those on buprenorphine maintenance (which is complicated due to buprenorphine's very high affinity for the mu-opioid receptor as well as its potential to cause acute opioid withdrawal). This is an area in which I personally have very little experience, and so I learned a lot, and would recommend the article as a primer on the topic.
Friday, January 20, 2006
Tuesday, January 17, 2006
Tuesday, January 17, 2006
Saturday, January 14, 2006
The current Journal of the American Geriatrics Society has a study on ICU mortality for those 90 years old & older. It is a prospective cohort study in a single Greek ICU comparing mortality for those over 90 with other patients. ICU mortality for the oldest was 20%, and 30 day in-hospital mortality was 40% (compared to 7% and 9%, respectively, for those under 90 years old). Interestingly, ICU mortality for those in their 80's was 11%, half of that for those in the next decade. Functional status for those who left the hospital alive was not measured, although most were discharged home. APACHE II score was the only independent predictor of mortality for the oldest old.
The authors set this data against what they suggest is a movement to a priori deny ICU care to the oldest old as a cost/resource savings measure. If this movement, in any organized or serious form, actually exists anywhere I'd be curious to see. They conclude that age alone can't be used to deny people ICU care because these outcomes aren't all that bad. Well, yes & no. Advanced age does carry with it a much higher risk of mortality ( 4.5 times higher in this study!), and if one were to ration ICU services based on likelihood of benefit then age would need be part of this mix. But if one were to do this then APACHE II scores would probably need to be a part of this mix as well, as the APACHE II strongly predicts mortality. This would then lead to an argument of denying ICU care to those who are sickest--who need it the most--which is ridiculous. The issue then, which strikes me as a false one, is the idea of denying ICU services to any broad group of people a priori. Use of the ICU--or any medical intervention--should be decided individually, based on an individual's comorbidities (including age), severity of illness, goals of care, and values. This is harder, messier, and more labor-intensive than the use of demographics as a clinical decision-making tool, but that's a good thing in my opinion.
Saturday, January 14, 2006
Thursday, January 12, 2006
Thursday, January 12, 2006
Tuesday, January 10, 2006
I've been sick, and so have taken the time to toy with Pallimed's layout.
Now, in the sidebar on the right, all of Pallimed's posts are listed in reverse chronological order. This will hopefully allow casual & new readers find older posts more easily, without having to dig through the archives. It also reinforced to me the folly of giving posts vague names like "Many articles" or "September's Gerontologist," as this forces the reader to open a webpage to find out if s/he wants to read the post. So I will stop doing that. I also created a new section of 'highlighted posts' which will have links to posts with information about the blog and anything else I decide to put in there.
I hope this will improve the accessibility of the blog. Let me know if you've got any further suggestions to improve the blog, or any other general comments.
Tuesday, January 10, 2006
There are two more articles from December's Journal of Pain & Symptom Management that I wanted to highlight.
First, there's a brief piece about using propofol as an anti-emetic and sedative in palliative care. It's essentially a case series of 35 patients in a palliative care unit who received propofol over 10 years in Stockholm. I'm not going to make much of its use in palliative sedation--it seems to work, the authors show their dosing data, it's probably no more or less dangerous that palliative sedation with benzodiazepines or barbituates. What is more interesting is their use of it to treat refractory nausea/vomiting. They present experience from 13 patients whose nausea persisted despite most typical antiemetics being thrown at them. In only 3/13 was treatement limited by excessive sedation, and most of the rest had good control of nausea with propofol without dose-limiting sedation. Doses were generally less than 1mg/kg/hour, and the authors recommended starting at 0.5mg/kg/hour and titrating to effect. (Be warned: data was not collected prospectively or in an organized/standardized fashion for this case series--my overall take on this data is that it's proof of principle for propofol as an antiemetic but not much more).
Second, long acting octreotide is examined for malignant bowel obstruction for ovarian cancer. The findings aren't promising, but this study is so small and preliminary that really no conclusions can be drawn. This was a pilot trial on 13 people with advanced ovarian cancer and bowel obstruction (however, 5 of them didn't evidence of bowel obstruction when imaged!) who were ineligible for surgery. They received the "depo" form of octreotide. Results were a complete wash--over half had no evidence of response. 3 patients did remain on it for more than 8 months leading the authors to remark about its "safety and tolerability," which is swell, but "efficacy" is important also. The study is so small, and the patient population probably poorly chosen, that by no means can long acting octreotide be written off, although its use currently can't be endorsed outside of a trial either, especially when there's at least some decent, positive data for short acting octreotide.
December's Journal of Pain and Symptom Management has a piece examining concordance between patients' and surrogates' understanding of end of life wishes. This is a large study for the field, involving 92 hospice patients and their surrogates (mostly spouses/partners or adult children). Both were asked extensive questions regarding end of life wishes (goals, hopes, concerns, priorities, etc). Agreement between patients and their surrogates was generally poor; among other findings most surrogates misidentified most patients' top priorities.
These are the general findings, but I'll warn you that this study generated mounds of data & one really begins to wonder how best to interpret them. I'll elaborate with a little research methods/epistemology detour. 31 end of life 'preferences' were measured for the study (everything from 'pain under control,' to 'time [spent] with pets,' to avoiding 'ventilator/dialysis to prolong life.'). If the fundamental question being asked is 'how good are surrogates at knowing patients' end of life wishes?,' how does one go about interpreting the data generated from these 30 questions? Is 50% concordance between answers to the survey "good"? 75%? 90%? Who decides? How do we decide if 90% vs, say, 50% concordance between surrogates and patients is a meaningful difference upon which we should act to improve the quality of of end of life care? And does it make sense to weigh all preferences equally? Is 'time with pets' equally necessary to "good" concordance between surrogate & patient as "say goodbye to loved ones?" Probably not. That is why the authors looked at agreement between what patients and surrogates viewed as top priorities.
I am not pointing this out to criticize the study; in fact the authors are quite upfront about these problems in the paper, and there's not like there's some standard out there they can turn to. What I do think is tough to justify 'scientifically' though is that the authors decided to define concordance as agreement within 1 point of 0-10 scale (in the survey the participants rated how important they thought something was on a 0-10 scale). So if someone rated 'dying in place of one's choice' as a 9/10 in importance but their spouse rated it a 7/10 the spouse's response was considered not in agreement. This seems arbitrary and tough to justify. Obviously the authors needed to pick a cut-off somewhere, but their findings would have been even more compelling if they showed their findings were valid even using different cut-offs.
Nevertheless the overall mediocre concordance between patient and surrogate throughout the study was so consistent that the 'big message' from the study resonates loud and clear: don't assume surrogates understand patients' wishes. As a bright note, however, the authors found that concordance between patients' and surrogates' answers was significantly improved if 1) the patient thought the surrogate actually knew their preferences, and 2) the patient reported talking with surrogates about treatment preferences. Seems obvious, but in fact this is not necessarily so given that all the rest of the study's findings demonstrate people don't understand loved ones' wishes as well as they probably think they do. So it's encouraging that we actually have some evidence to say if people actually talk about this, understanding is improved. The other 'big message' then is a reminder to us clinicians to facilitate these discussions.
(There's also an article looking at a Taiwanese population, finding that families' end of life preferences for patients are usually more 'aggressive' than the patients' own wishes.)
New PC-FACS are out. My prior comments stand: superb, wish they were free to all.
I'll be blogging about a couple other pieces of Decembers JPSM later this week.
Thursday, January 5, 2006
The Journal of General Internal Medicine has an intriguing article about predictors of the loss of decision making capacity in demented patients. To be clear, I did not find the article intriguing because of their findings of what predicted loss of decision making capacity; that was a lot of technical neuropsychiatric stuff that I don't understand. Instead, what was intriguing was that the study followed demented patients longitudinally (over 9 months) and assessed capacity over that time. The study looked at 53 elderly people who were in a study on decision making capacity & who, during screening for the study, were found to have dementia (it's unclear whether or not they had previously been diagnosed with dementia). These 53 had mild or moderate dementia--not severe. They assessed decisionality with some battery of neuropsych testing at baseline and then at 9 months. Initially 9% of the group lacked decision making capacity; after 9 months 26% did. This is interesting for what it says about the natural history of dementia, but also for how imperative early and comprehensive advanced care planning is for those with dementia, given how rather quickly decision making capacity was lost in this population.
Thursday, January 5, 2006
The current New England Journal of Medicine has a perspectives piece by Timothy Quill and Diane Meier about the upcoming Supreme Court decision regarding the Oregon physician assisted suicide law (and whether the DEA or the state medical boards have the power to restrict physicians' use of controlled substances). Their take is that a decision in favor of the DEA will have a chilling affect on physicians' prescribing of controlled substances to dying patients, for fear of scrutiny for being involved in 'assisted suicide.' It is a chilling article and all I can say is that if the Supreme Court rules "against" the Oregon law, I hope Drs. Quill andMeier are wrong. A quote:
This type of DEA involvement in medical practice would adversely affect far more patients than those few who seek assistance with a hastened death in Oregon. If the government thus oversteps its legitimate role and expertise, allowing DEA agents, trained only to combat criminal substance abuse and diversion, to dictate to physicians what constitutes acceptable medical practice for seriously ill and dying persons, it will undermine palliative care and pain management for the much larger number of seriously ill patients in all states.
Free full-text is available.
Tuesday, January 3, 2006
BMJ has published a piece about coma prognosis for characters on soap operas (along the lines of the famous article about CPR outcomes on the TV show "ER" 10 years ago). They looked at 10 years of programs from 9 popular US soaps. I can't vouch for how good these results are as the authors were forced to use non-validated secondary sources for their findings & it appeared they came across some unusual methodological contingencies. A quote:
We included only the first episode of coma for each patient. We determined the patient's characteristics and the cause of coma by reviewing the storyline at an official or sanctioned website and resolved disagreement by consensus. When a patient had an identity change (a facial transplant in one case), we used the characteristics of the original patient for analysis.
The results are not surprising. Notably, 89% of patients recovered fully, and 86% of patients had no residual disability on the day that they recovered (except for, naturally, some amnesia). This, the authors point out, is for a population (soap opera characters) that has a remarkably high overall mortality.
They conclude: In the interests of public health, soap operas and other forms of mass media should seek to balance stories of improbable survival and recovery with compelling and compassionate stories of characters who die with comfort and dignity.
Good luck....
(BMJ annually publishes an issue devoted to unusual and unconventional papers, often--but not always--funny, & this article is from this year's. It's worth a read if you have the time.)
Tuesday, January 3, 2006
Happy New Year Pallimed readers!
Pain has an interesting article on the diurnal variation in chronic neuropathic pain. It caught my eye because I was taught, & I think many people believe, that pain tends to be worse at night. I always attributed it to people being less busy at night, with more time to notice their pain, but clearly that's just a gross assumption that may not be true at all.
The Pain article looks at data gathered from the randomized controlled trial comparing morphine to gabapentin for chronic neuropathic pain (diabetic neuropathy and postherpetic neuralgia) that was published last year in the New England Journal of Medicine. For this article they looked at the pain diaries for the patients when they weren't receiving any active therapy & found a distinct increase in pain across the day. The figure shows the diabetic neuropathy results--you can see quite vividly that the 8pm pain scores were consistently and predictably worse, by a sizable 2/10 points on the 0-10 numeric rating scale, than the 8am scores.
They found similar results for PHN, although the magnitude of the swing wasn't as pronounced. This pattern was preserved even when people were on active treatment. Pain scores overnight (8pm to 8am) weren't, unfortunately, recorded for the trial.
Why this happens I don't know. In their discussion, the authors make murmurings about circadian fluctuations in neurotransmitters and endorphins, and ask whether melatonin (which increases at night) is pro-nociceptive. Clearly, however, no one knows--nor is it known how significant this is outside of chronic neuropathic pain--but the figure dramatically displays how real a phenomenon this can be.