

Tuesday, January 31, 2006
Breaking bad news; Multidisciplinary approach doesn't necessarily make cancer suck any less
The current Journal of Clinical Oncology has a couple articles to note.
First, there is a discussion of recommendations for breaking bad news. It is based on data that is being gathered for a larger trial about communication in oncology clinics, and uses information coded from video-taped encounters between oncologists and patients. The authors present their discussion against a straw-man of pre-existing 'guidelines' about breaking bad news which they suggest are overly simplistic. Obviously they are overly simplistic--that's the nature of guidelines--but the authors' observations about how bad news unfolds in the clinical encounter are nonetheless interesting and useful. First, they observe that 'bad news'--defined as " [news that] results in a cognitive, behavioral, or emotional deficit in the person receiving the news that persists for some time after the news is received"--comes out all the time in routine clinical encounters (not just in the You Have Cancer or You Are Dying talks). Second, they point out that to patients and families there's sometimes not a central Bit of Bad News, but rather several (3.2 on average per encounter, actually!) pieces of 'bad' information that come out in an encounter. Finally, they observed that a physician-patient dyad doesn't really exist, and that family members often contribute as much to the encounter as patients or docs. None of this is earth-shattering; but it's interesting to see data taken from actual physician-patient-family interactions. I'm not clear what the goal of the larger trial is, but based on this preliminary missive, it seems that its results may be quite interesting. I guess we'll wait and see.
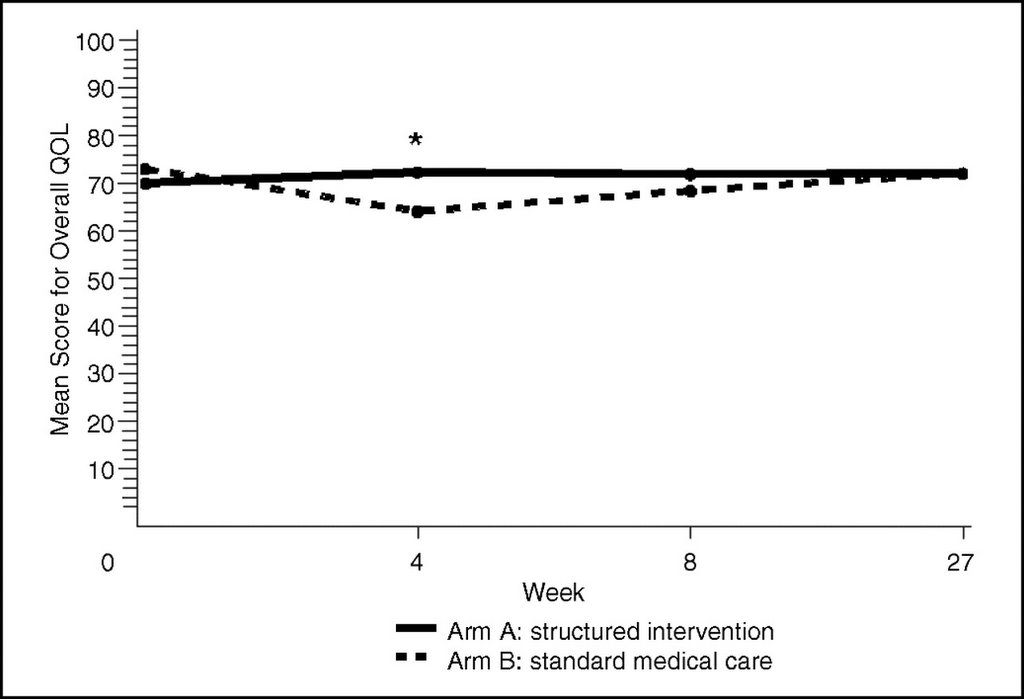
Additionally, a randomized-controlled trial about a multidisciplinary intervention to improve the quality of life for 'advanced' cancer patients is presented. This was a trial at Mayo for patients with advanced cancer (defined as life expectancy longer than 6 months but mortality at 5 years thought to be over 50%) undergoing radiation therapy. The treatment group received a multidisciplinary intervention (8 sessions, 90 minutes each, over 3 weeks) comprising physical therapy, chaplaincy services, and broad ranging cognitive-behavioral-emotional education and support. Essentially, the intervention group did a little better quality-of-life-wise at 4 weeks but this quickly petered out; mostly this benefit was in stopping the decline in quality of life during radiation treatment that the control group experienced. See the figure below...despite statistical significance not a very impressive response.
This is one of those articles that if you read the abstract you get the feeling that this was a solid success, whereupon reading the text you realize that it the intervention's benefit was modest (at best) and transient (and at what cost?). My gloss on this is that the problem may be one of selection--services like this are probably only helpful for a subset of patients and the trick may be in figuring out which ones. Part of what I'm suggesting is that for many patients 'quality of life' is adversely affected by so many things that these sorts of interventions just can't address. Having advanced cancer sucks (as many buttons worn by staff at the cancer center I work at attest to); it makes you feel crappy and usually eventually takes everything meaningful away from you including your life. Benefits aside--cancer treatment, radiation included, also sucks and makes you feel crappy while you're undergoing it. Will having sessions discussing body image and stair exercises make this suck any less? For many people clearly not; the trick is to identify those for whom it would help.
(& I did listen to the Fresh Air bit from earlier this week & it's quite good: a short, fluent, and sometimes personal account of geriatric and end of life care in 21st century America.)

